An In-Depth Look at Graft Versus Host Disease (GVHD)

Over the last five years, progress in GVHD understanding has redefined the GVH reaction and created new possibilities for novel preventive and therapeutic treatment innovations. The advancement in the immunology field has widened the new possibilities for hematopoietic stem cell transplant. This has led to the availability of different stem cell sources for possible grafts and the adoption of novel conditioning regimens. Although numerous transplant centers have adopted various preventive modalities, no standardized regimen remains. As for now, immunosuppression using steroids is the first line of intervention. Treatment for steroid-refractory GVHD, including mesenchymal stem cells, anti-thymocyte globulin, and extracorporeal Photopheresis, is being investigated with various novel, innovative therapeutic therapies.
What Is GVHD?
When the transplant graft’s immune cells identify the host as alien and attack the recipient’s body cells, this results in Graft-versus-host disorder. It is a typical adverse event after the allogeneic hematopoietic stem cell transplant. Based on the timing of onset, a cutoff of 100 days post-transplant GVHD can be classified into below types:
- Acute GVHD: Within the first 100 days post-transplant with typical clinical signs of acute GVHD such as skin rashes, liver dysfunction, and gastrointestinal issues such as diarrhea and abdominal pain
- Chronic GVHD: This can manifest with the typical clinical characteristics of chronic GVHD, such as dry eyes and mouth, joint stiffness, and skin thickening after the first 100 days, and may persist for months or years.
- Persistent or Recurrent or Late-Onset Acute GVHD: Appears with clinical signs of traditional acute GVHD but after 100 days of transplantation.
Overlap syndrome may present features of both acute and chronic GVHD at any time post-transplant.
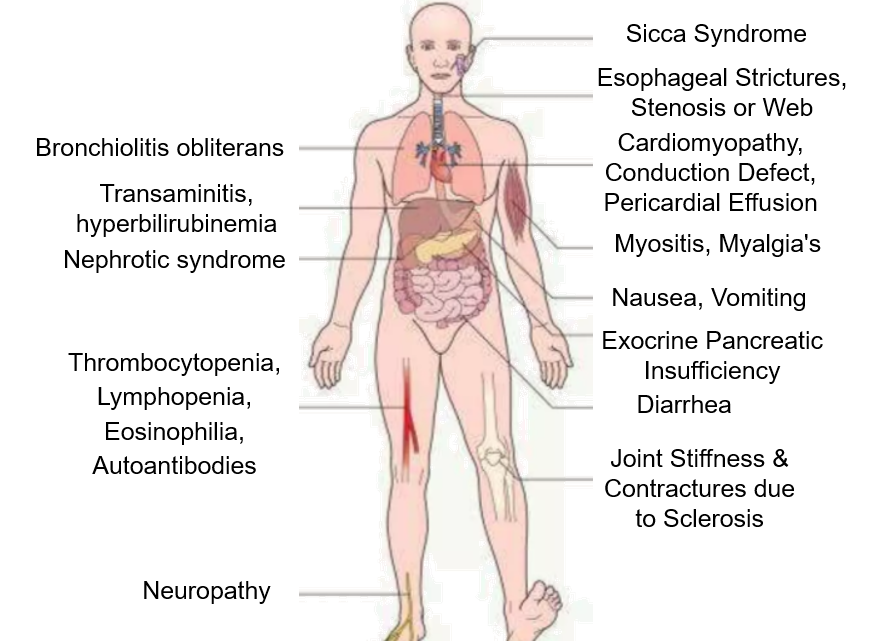
Figure 1: Multi-organ Manifestations of Chronic GVHD
Factors for GVHD Occurrence and Severity
- Donor-Recipient Factors: Increase in GVHD incidence with unmatched donor transplants, HLA disparity, and sex mismatching
- Origin of Stem Cells: Among the sources that can produce stem cells, the use of umbilical cord blood or bone marrow lowers the GVHD incidence
- Aging: Individuals with pre-existing morbidities and older recipients have a higher risk of developing severe GVHD.
- Immune Modulation Factors: GVHD incidence is lower with triple therapy (cyclosporine, methotrexate (MTX), and prednisone as compared with double therapy (cyclosporine and MTX). Statins can inhibit APC function and reduce MHC class II expression in the pre-clinical setting
- Chemotherapy and Radiation Therapy: An excessive dose of chemotherapy damages nearby tissue and increases the circulating cytokines levels, leading to a cytokine storm. This increases the graft’s immune cells’ capacity to recognize host antigens.
The GVHD is less understood due to its intricate mechanism. It can also occur in autologous form, usually after a peripheral blood stem cell (PBSC) transplant.
Figure 2: GVHD Mechanism
Global GVHD Market
Due to the increasing number of stem cell transplants, the GVHD market is expected to grow rapidly in upcoming years. Immunosuppressants dominated the market due to their ready availability as over-the-counter drugs. It is projected that biologics will lead the future GVHD treatment market, as opposed to small molecules.
North America holds the largest share and dominates the market owing to an increase in the number of organ donations of deceased persons for transplantation, an increase in the allogenic transplantation procedure, and a surge in the number of cancer patients in this region.
APAC region is expected to grow quickly due to the Rise in the geriatric population. Therefore, the need for transplants will eventually lead to increased demand for drugs such as corticosteroids and monoclonal antibodies for GVHD treatment.
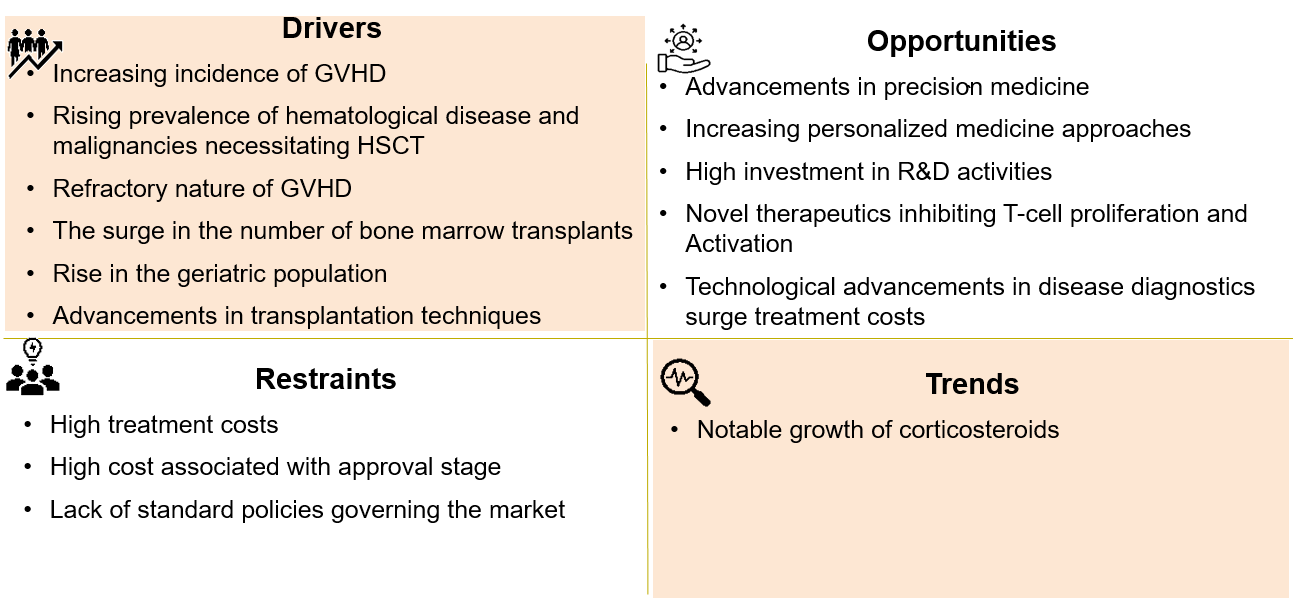
Figure 3: GVHD Market Dynamics
Ecosystem
While Latin America, the Middle East, and Africa are still facing some challenges related to inadequate healthcare infrastructure and low awareness, the United States has well-settled transplant centers and a well-functioning clinical trial industry.
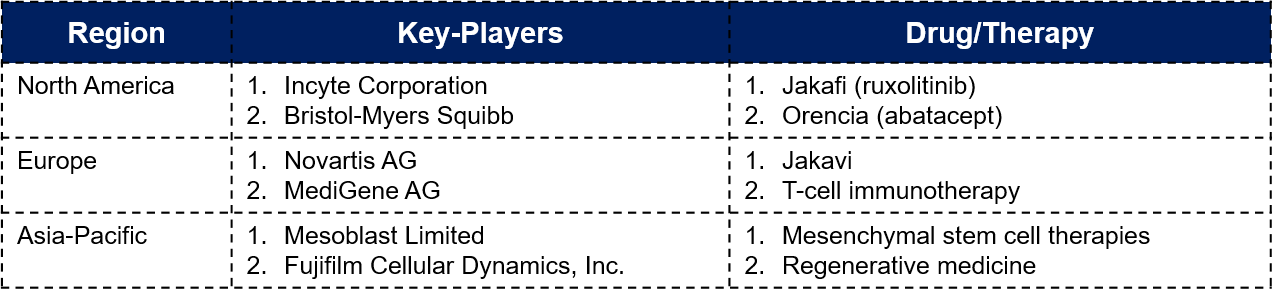
Figure 4: Region-wise Key-Players and Their Drugs/Therapy
In 2021, Sanofi acquired Kadmon Holdings to strengthen the growth of the transplant business by adding REZUROCK to its transplant portfolio.
In 2022, Novartis obtained European Commission approval for Jakavi’s use in patients aged 12 and older with acute or chronic GVHD who have not responded to corticosteroids or other systemic treatments, offering novel therapeutic therapies.

Figure 5: GVHD Market Key Players
What’s New in the GVHD Domain – Upcoming Technologies
Novel development, technological advancement, and ongoing research are rapidly improving the diagnosis, prevention, and treatment of GVHD. Following are some of the latest technologies and upcoming approaches in the GVHD domain:
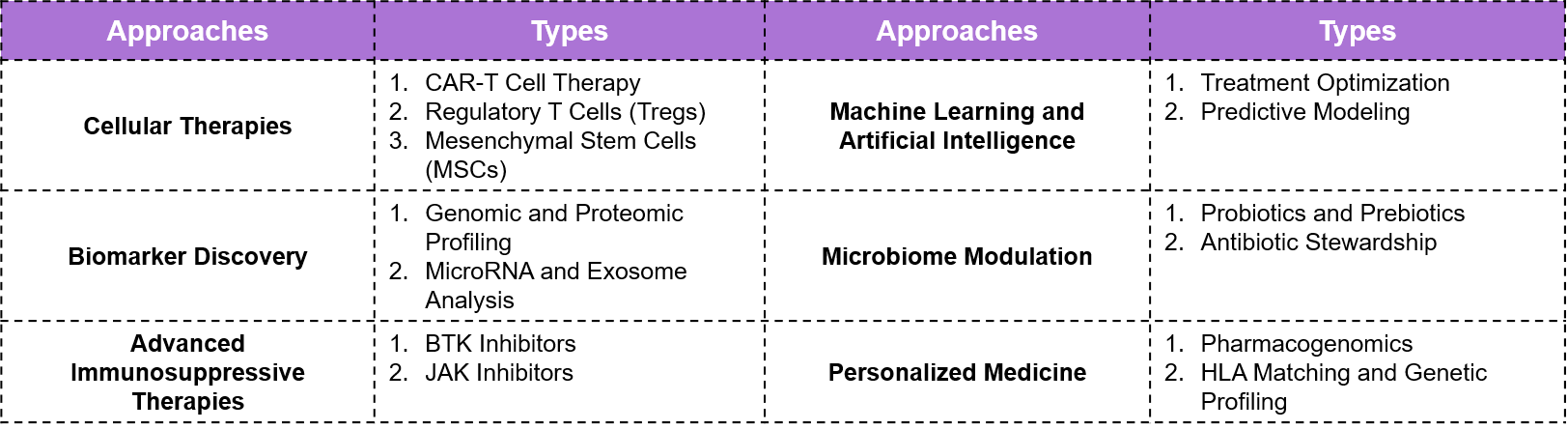
Figure 6: Latest Technologies and Upcoming Approaches
Future Prospective and Conclusion
GVHD still has various risks. To improve treatment and results, individuals around the world are continuously working on novel technologies. With the help of ongoing research and new therapeutic approaches, the success rate of stem cell and bone marrow transplants can be increased. The future of GVHD treatments will depend on personalized medicine, immunosuppressive strategies, and cellular therapies. Collaboration and investment in healthcare infrastructure are necessary to ensure that treatments are accessible to patients worldwide.
Let's Take the Conversation Forward
Reach out to Stellarix experts for tailored solutions to streamline your operations and achieve
measurable business excellence.